
There is still benefit for many people who take SSRIs and other antidepressants/antianxiety. I have found sertraline to be pretty helpful, personally. That said, this review is consistent with the notion that depression is not simply a serotonin deficiency. I've seen some arguments that neurotransmitter reuptake inhibitors work for more complicated chemical reasons because of the way that serotonin and other neurotransmitters interact with each other. I've also heard the argument that while SSRIs are good, it's no better than a true active placebo that mimics the side effects of an SSRI. I'm certainly not a medical expert, but I'd caution against telling people that a medicine someone is taking is actually doing nothing. It's not uh...it's not really what you want to hear someone else put on you, especially for political reasons. Much better I think to simply acknowledge that the drugs can help some people's symptoms, and then pivot into the myriad social material causes of depression and anxiety, namely being human in an inhuman capitalist hellscape.
IIRC, antidepressants work better for worse conditions, while barely helping mild depressions.
That would make a lot of sense to me. I'll also add for what it's worth that I only tried them because I was at my wits end and talk therapy wasn't helping my feelings of constant guilt at living within the imperial core.
For sure. I heard a doctor put it well "A headache isn't caused by a paracetamol deficiency, but that doesn't mean it won't help.".
If such antidepressants are helpful for you, then by all means go for it. We can treat the symptoms while still fighting to cure the root problem.
Especially when the symptoms so often leave you unable to do anything. I'd rather be able to actually decide to fight the system than not have the choice and have to sit and do nothing.
Oh weird! could it be that rates of depression are higher in more fucked up societies and among more oppressed groups within those fucked up societies? and that it’s not just brain chemicals but also the social environment that causes depression/anxiety/etc that are rampant in the USA?!? And that allowing tons of chemicals in our food/water/air/etc might contribute to it too? But that no one wants to talk about those causes because the solution is social and policy change and not medical?
DUHHHHH.
Capitalism is the cause.
Communism is the cure.
Simple as.
This has been known for more than a decade (this study is just a review of existing research), and is not directly related to the efficacy of SSRIs (although the serotonin "theory" might have led to their adoption, idk).
For a while now, as I understand it, the view has been that SSRIs cause the downregulation (decreased new production of) serotonin receptors in reaction to the excess serotonin buildup they cause in the synapses (this is why they take a few weeks to kick in, despite increasing serotonin levels almost immediately, and is also why they will desensitive you to psychedelics like LSD, which act primarily on serotonin receptors). They decrease overall serotonin signalling, which in turn has downstream effects that alter certain activites of certain regions of the brain that are implicated in depression. (This is based mostly on discussions I had with my psychiatrist a few months ago, so if there are any actual experts here, correct me if I'm wrong.)
That being said, SSRIs suck ass, their side effects are awful, and I think it's medical malpractice to make them a first-line treatment tbh. It's really mind-boggling that they're the go-to given how much shit they fuck up.
That being said, SSRIs suck ass, their side effects are awful, and I think it’s medical malpractice to make them a first-line treatment tbh
I love reading about their effects on libido including doctors "joking" to women about how they won't need birth control anymore (due to lack of desire for sex) and such side effects can last years after discontinuation very cool definitely not fucked up
growing up in my 20's thinking i was ace but it was that or constantly wanting to redact myself, shoutout to ssri's i guess
My ex and I taking SSRIs ultimately led to our breakup. The libido thing is no joke.
My SO's libido has been fucked for like 6 years now. She took Zoloft for like, one year
This is just one anecdote, but for me starting an SSRI was incredible. The start up period was rough, but once I got used to it I had almost no side effects and my panic attacks went from weekly to annual. I understand that this isn't everyone's experience though.
I don't doubt it. They do sometimes work, which is why I don't like the way this paper is being passed around; people are drawing incorrect conclusions from it.
That being said, here's my anecdote: I was worried about the side effects and hesistant to try them, but everyone dismissed my concerns, insisting that SSRIs are the "gold standard", that they're the most effective, that the side effects usually aren't too severe, blah blah blah. But not only did everything I worried about happening happen, they also did absolutely nothing to help me. I would rather have wasted my time with bupropion or some other drug that didn't fuck my shit up at all. Drugs with less severe and less frequent side effects should be tried first (that's usually the standard in medicine!). I believe the pharmaceutical industry has had a hand in this, and I think it constitutes systematic malpractice.
Yes. No. Maybe. Different people react differently to them. Lots of people tolerate them with no side effects, other people have terrible side effects. As far as I know there's no way to tell who will and who won't respond well to them, though I think there are now some genetic testing techniques that can help figure out which medications are more likely to work.
I dunno, I've been taking an SSRI for a while and they've worked pretty well for mellowing out my anxiety and depression. I am planning on stopping taking them eventually, especially when i go to get some ADHD meds.
I dont really care if its an imbalance or not life without sertraline would be unlivable for me
Change my life. Gave me the ability to understand the breadth of my illness. And allowed me to point out abuse I had been tolerating from family members who suffer from the same condition but refuse to seek help.
Very similar experience for me, I was finally able to separate the illness from my own personality whereas over a decade prior i could not discern between the two
It still happen on occasion, but now I know. I call it my brain trying to eat me.
Exactly, the first break thru I had on the drugs were when something happened and a thought entered my head that normally would tie me into knots, just was a brief thought and went away. Like holy shit I was fucked up!
Ynow im happy to talk to someone with the same experience as me. I had the same family, refuse treatment and also convinced me to never get treatment and we all made each other miserable dragging each other down.
Too true. Sure glad as well. I'm glad you found help. The American health system is a strange sea to navigate.
I hope you're able to manage your family. And keep healthy boundaries.
i can tell you right now that all the anxiety and ptsd related meds ive taken have done jack shit (and in many cases made it worse), and the only thing thats ever helped me were sleep meds. and ive swapped through well over 2 dozen kinds of pills for it. therapists are even more useless for me. sleep meds dont get rid of it but it makes the nightmares go away which has a positive cascading effect on my mood and anxiety. also makes me not shatter my teeth in my sleep
Have you ever tried pregabalin? It kind of exists in an efficacy sweet spot where the risk of bad withdrawal is less than with benzos and Z drugs, while still providing relief from panic attacks.
yeah been on it before cause of nerve damage flares and also for anxiety, no change. in fact i think thats one of the ones that made it feel like i chugged 20 cups of coffee
Damn. Are you really caffeine sensitive? I can have just one cup of coffee and it will be enough to send me into a dissociative state. Even iced tea can mess me up.
im like, really tiny, so more like im sensitive to everything lmao. ive already tried cutting meds too.
yeah since stuff like NMDA receptor antagonists like ketamine do such wonders for short term depression relief there is a far more complex neurochemical pathway involved (if it's even purely neurochemical at all which i have always been suspicious of)
The discussion around this sounds a lot like the discussion around ADHD medication and how people compare it to meth or think it's a scheme by pharmaceutical companies. Whatever the cause is, SSRI's have helped a lot of people turn their life around and improve themselves, while other cases it did nothing and maybe made things worse.
good thing to hear after finally starting taking some antidepressants :agony-shivering: . At least therapy works for me I guess
Doesn't mean that it doesn't work, just means it's more complicated. Antidepressants cause a statistical significant improvement in peoples lives.
The article doesn't actually say much that is interesting or useful. Everyone in the field knows that the "Chemical Imbalance" thing is bunk. SSRIs still work really well for a lot of people, don't let one meta-study by some people with a point to prove turn you off if they're working for you.
:shrug-outta-hecks:
I think most of them stick to only medical subreddits though
This is saying, "Actual psychiatrists have known this for nearly twenty years, so there's no reason for it to be making news and no one should care." :so-true:
Too bad fuckin no one else seemed to know this.
Ok but people seem to be taking this study to mean that ssri's don't do jack shit. If the people who prescribe them knew about this and still prescribe them then they still probably do something.
Good point. For many people, myself included, SSRI's don't do jack shit. I understand that they help a lot of people. It just sucks that they're always the first line of treatment that professionals I've seen go to (and in my childishness I stop seeing them and get no treatment whatsoever).
One possible interpretation here is that "depression" is a cluster term that describes symptoms rather than pathologies. Something similar is true of (among other things) psychosis, which is a symptomatic cluster that can have a broad spectrum of proximal causes.
Philosophy of mind isn't my specialty, but I know enough about it to have a strong suspicion that in another few decades, we're going to view diagnoses like "depression" similarly to how we view 19th century diagnoses of "hysteria" now: clusters of symptoms that were complex, multifarious, and socially influenced in both etiology and appropriate treatment.
Yeah the "chemical imbalance" theory of mental health was literally made up by an advertising agency.
They thought, correctly I imagine, that people would be more likely to take medicine for it if they had a simple theory like that
Unlikely. This isn't anything new and the authors of the study are sketchy as hell.
but where will I buy snarky one-dimensional T-shirts that attribute my happiness (or lack thereof) to one single molecule in an attempt to be nerdy and stuff?
I had it bad, like almost 0 functioning ability, and nothing worked before ketamine. So personally checks out.
I read one reason ssris could still work for some people is because for one they are actually pretty good at reducing anxiety symptoms, but also just because serotonin deficiency isn't the cause of depression doesn't mean that increasing serotonin can't improve your mood at all.
I’m so pissed, my insurance company refused to approve ketamine for me for some fucking reason. I’ve tried tons of different anti-depressants and nothing has worked.
Hey! Would be curious about your experience with ketamine. My partner is looking to get treatment. Personally I've done tons of mushrooms , a little LSD, but never ketamine. Shes used mushrooms once and it was really difficult but ultimately healing (her words). She's resistant to trying SSRIs entirely (i support this 100%) and is looking for alternatives to approaches that medicalize/pathologize trauma.
To start I have to say it can be pretty expensive. I'm in the US and insurance won't cover it, they can't get IV ketamine "approved" for depression because there's no money to be made off the drug itself because of how old it is. It's one of the cheapest drugs to make so the money is just for the people watching you sit there I guess. There's nasal spray "esketamine" which my doctors don't recommend bc with IV its easier to control the dose, that got approved because it has a patent, so it's technically possible to get that covered but in my experience providers of that also choose to not take insurance.
I'm sure you could find a doctor with any kind of opinion but mostly they don't use it as a first line of treatment because of how involved it is. So I'm not sure if someone who hasn't been on any antidepressants before would have good chances getting it prescribed. A couple years ago I read a lot of things where they were recommending it to treatment resistant patients mostly, which is 3+ meds unsuccessful. Also most doctors will want you to be on another antidepressant aside from the ketamine. I stopped taking mine without mentioning it because it wasn't doing anything. lol
As for the actual treatment. It takes like an hour and they give you a little bit every 10 minutes or so and then just let you sit until you're good to leave. It's an anesthetic so she should have someone go with her because she'll probably be disoriented for a little bit. The half life is very short though so any side effects should be gone within a couple hours. I've seen people online talk about it like being high or about "k holes" or w/e but I think they're being dramatic. When I get it I feel a little out of it, kinda physically numb, and the room does look a bit strange as if the distance between everything and/or size of objects has been altered slightly, but nothing too serious. You mentioned she has trauma. If she has any significant amount of dissociative symptoms from that then her brain probably hits her with way more heavy experiences than the small amount of ketamine would, at least that's how it is for me. I usually text or read things online the whole time idk.
Symptom relief is pretty immediate. Your mood improves within a few hours usually. For people currently in an episode getting treatment for the first time they get a bunch of treatments every few days for a couple weeks. It's not always long lasting, some studies say there's a drop off after like 2 weeks no treatment. But most doctors that do it say people can usually start spreading out appointments much longer than that. I get a headache afterwards until I sleep it off so usually I notice the difference in symptoms from when I wake up from that. lol Since I started it I can kinda enjoy things again whereas before treatment I had stopped bothering to even try playing video games anymore, and those things are designed to keep your constant attention with little dopamine hits. I can hold a job now, even if it's not always easy (I do have other physical and mental health issues so I can't say how much is lingering depression). I even can focus enough to read sometimes. No suicide attempts since, almost no self harm and if it was it from ptsd so it had a clear trigger. I remember to eat more often and take care of hygiene. I socialize more. Pretty much everything is much better, not perfect of course but yeah.
I think that about covers what I can say without being prompted by more specific questions. lol
I have been interested in trying ketamine for depression too.
And i was watching that news comedy YouTube thing with that guy Cody and he mentioned it was easy and cheap to get and you didn’t even need a prescription. So i looked around but couldn’t find it anywhere except those really expensive clinics that administer it like what you go to.
Do you or anyone know what Cody was talking about? Is there just like a way to order it online from like Mexico or something?
I go to a psychiatrist's office, you might be thinking of a ketamine clinic. I have no experience with those. I tried looking into them and saw a bunch of stuff about shady doctors that got arrested and kinda got too nervous about messing with my treatment like that when I know it works currently.
I don't know who Cody is, but I know the other way to get it aside from psychs and specific ketamine clinics is through a pain management doctor. That still needs a prescription though. Again at least in the US, I really can't speak about other countries. The pain management route seems somewhat easier, chronic pain doesn't always have a specific diagnosis to it so you can probably find places where you just get an appointment and ask about it.
Cody is the guy from some more news https://youtube.com/channel/UCvlj0IzjSnNoduQF0l3VGng
Yeah i was talking about a ketamine clinic. They have one at the same place where my partner gets her medical weed card. Lol.
Thanks for the info.
I’ve seen people online talk about it like being high or about “k holes” or w/e but I think they’re being dramatic. When I get it I feel a little out of it, kinda physically numb, and the room does look a bit strange as if the distance between everything and/or size of objects has been altered slightly, but nothing too serious.
I had a very marked "trip" when I did IV ketamine treatment. It's hard to describe but it was not subtle or mild. Not unpleasant or upsetting, either, but it was a very obviously altered state of mind. I mostly just listened to music while I was doing it. Pink Floyd goes really well with tripping balls on sanctioned IV Ketamine.
Abstract
with highlights
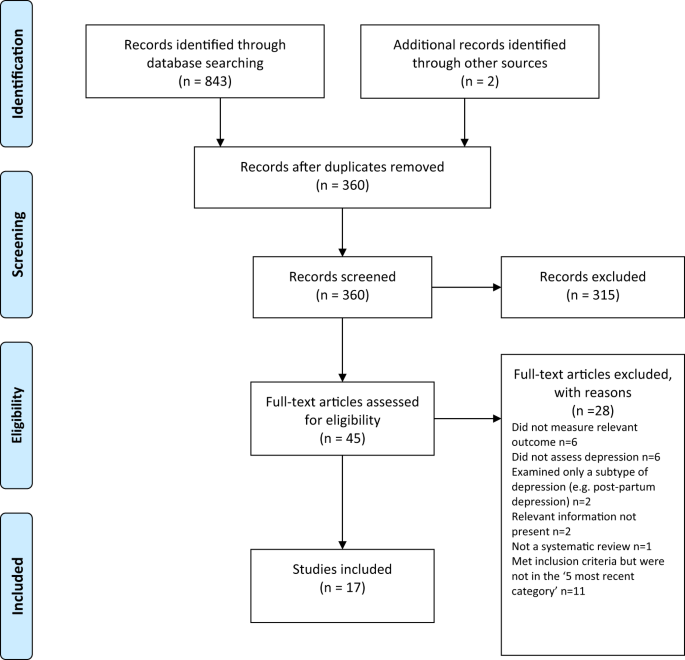
The serotonin hypothesis of depression is still influential. We aimed to synthesise and evaluate evidence on whether depression is associated with lowered serotonin concentration or activity in a systematic umbrella review of the principal relevant areas of research.PubMed, EMBASE and PsycINFO were searched using terms appropriate to each area of research, from their inception until December 2020. Systematic reviews, meta-analyses and large data-set analyses in the following areas were identified: serotonin and serotonin metabolite, 5-HIAA, concentrations in body fluids; serotonin 5-HT1A receptor binding; serotonin transporter (SERT) levels measured by imaging or at post-mortem; tryptophan depletion studies; SERT gene associations and SERT gene-environment interactions.Studies of depression associated with physical conditions and specific subtypes of depression (e.g. bipolar depression) were excluded.Two independent reviewers extracted the data and assessed the quality of included studies using the AMSTAR-2, an adapted AMSTAR-2, or the STREGA for a large genetic study. The certainty of study results was assessed using a modified version of the GRADE. We did not synthesise results of individual meta-analyses because they included overlapping studies. The review was registered with PROSPERO (CRD42020207203). 17 studies were included: 12 systematic reviews and meta-analyses, 1 collaborative meta-analysis, 1 meta-analysis of large cohort studies, 1 systematic review and narrative synthesis, 1 genetic association study and 1 umbrella review. Quality of reviews was variable with some genetic studies of high quality.Two meta-analyses of overlapping studies examining the serotonin metabolite, 5-HIAA, showed no association with depression (largest n = 1002). One meta-analysis of cohort studies of plasma serotonin showed no relationship with depression, and evidence that lowered serotonin concentration was associated with antidepressant use (n = 1869). Two meta-analyses of overlapping studies examining the 5-HT1A receptor (largest n = 561), and three meta-analyses of overlapping studies examining SERT binding (largest n = 1845) showed weak and inconsistent evidence of reduced binding in some areas, which would be consistent with increased synaptic availability of serotonin in people with depression, if this was the original, causal abnormaly. However, effects of prior antidepressant use were not reliably excluded. One meta-analysis of tryptophan depletion studies found no effect in most healthy volunteers (n = 566), but weak evidence of an effect in those with a family history of depression (n = 75). Another systematic review (n = 342) and a sample of ten subsequent studies (n = 407) found no effect in volunteers.No systematic review of tryptophan depletion studies has been performed since 2007.The two largest and highest quality studies of the SERT gene, one genetic association study (n = 115,257) and one collaborative meta-analysis (n = 43,165), revealed no evidence of an association with depression, or of an interaction between genotype, stress and depression.The main areas of serotonin research provide no consistent evidence of there being an association between serotonin and depression, and no support for the hypothesis that depression is caused by lowered serotonin activity or concentrations. Some evidence was consistent with the possibility that long-term antidepressant use reduces serotonin concentration.